


3.6 Surgica l Sucti 49
Needle-holding forceps are purpose-built instruments, important features of which include:
●●A finger-ring handle design, for easy manoeuvrability in the oral cavity.
●●A ratchet, to allow the instrument to keep a fixed suture needle position without application of force.
●●A cross-hatched working surface, to allow the holding of a suture needle across a broad range of angulations.
These instruments allow for correct use of a suture needle, reducing the propensity for soft tissue trauma from excessive manipulation of the friable mucosa and gingiva. The most common design used in oral surgery is the Mayo-Hegar needle holder. A critical error made by the novice dentoalveolar surgeon is to use artery forceps instead, in order to avoid the additional cost of purchasing a needleholding instrument. This is dangerous, as artery forceps do not provide sufficient grip or control of the suture needle, which can lead to needle breakage or poor control when working in the oral cavity.
Gilles forceps are the instrument of choice for grasping periodontal tissues to assist with approximation and closure with sutures. They are ideal for the oral cavity given their straight profile, small size, narrow jaws, and cross-serrated tips, with teeth that can hold and grip the smooth and often lubricated periodontal tissues. Gilles forceps are held in a similar manner to a pen, with the thumb and forefinger controlling the tips of the instrument.
Whilst there is no particular scissor designed for suture cutting in the oral cavity, an appropriate suture scissor should have sufficient handle length to access the posterior oral cavity, short blades to avoid inadvertent damage to oral tissues, and a slight curve in the blade to facilitate visualisation of the suture being cut.
Sutures are available in a wide variety of materials, needle types, and sizes (Table 3.5). Generally, suture materials are classified based upon type of material (synthetic versus natural), ability to be resorbed by the tissues, size, and structure (monofilament versus braided). Whilst the type of suture used is largely dependent on surgeon preference, each characteristic has a significant effect on intraoperative handling and postoperative healing (Table 3.6). A mid-sized (3-0 or 4-0) resorbable suture on a 3/8″ circle needle is generally acceptable for use in minor dentoalveolar surgery (Figure 3.14).
3.6Surgical Suction
A good surgical suction device is an essential component of any dental extraction procedure, not only to provide access and visibility, but also as an important safety measure for emergency airway management. A fine (2 mm-diameter) Frasier-style suction tip, attached to a high-volume suction outlet, affords excellent manoeuvrability in the mouth and allows for rapid evacuation of surgical-site debris and fluid by the surgical assistant (Figure 3.15). Conventional lowand high-volume suction devices used in dentistry are not fit for the purpose of dentoalveolar surgery.
Table 3.5 Common suture materials used in the oral cavity,classified by behaviour and filament type.
Suture materials
|
Resorbable |
|
|
Nonresorbable |
||
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||
Monofilament |
Braided |
Monofilament |
Braided |
|||
|
|
|
|
|
|
|
Gut (plain or |
Poligecaprone 25 |
Polyglactin |
Polyglactin 910 |
Nylon Polypropylene |
Silk Polyester |
|
chromic) |
|
910 |
(rapid) |
|
|
|
|
|
|
|
|
|
|
https://t.me/DentalBooksWorld

503 Basic Surgical Instruments
Table 3.6 Characteristics of suture needles and materials.
Characteristic |
Types |
Effect on handling |
Needle size |
Suture needles may come in a variety |
|
of sizes, measured by the chord length |
|
between the tip and the swage |
Needle shape |
The shape of a suture needle is based |
|
on what proportion of a full circle its |
|
arc forms, expressed as a fraction; most |
|
commonly, needles are 1/2 or 3/8 arc |
Filament type |
Monofilament |
A smaller needle may be easier to manoeuvre in the oral cavity but more susceptible to deformation or breakage
The arc of a needle affects intraoperative handling; a greater arc may help take deeper tissue bites, but is harder to manoeuvre in smaller spaces
Smooth monofilaments pass through the tissues easily and do not elicit as great a tissue reaction, but are more difficult to tie due to knot slippage
|
Braided |
Rope-like braided filaments have better grip |
|
|
against tissues and are easy to tie, but may |
|
|
elicit a tissue reaction |
Filament |
Natural |
Natural filaments are degraded by proteolysis; |
material |
|
a tissue reaction is more likely |
|
Synthetic |
Synthetic filaments are degraded by enzymatic |
|
|
breakdown; a tissue reaction is less likely |
Absorbability |
Absorbable |
Absorbable sutures do not require secondary |
|
|
removal, but their duration of strength may be |
|
|
variable |
|
Nonabsorbable |
Nonabsorbable sutures require removal at a |
|
|
later stage, but their strength and hold are |
|
|
almost guaranteed during this time |
|
|
|
Figure 3.14 Front of a suture packet, detailing suture gauge (3-0), needle type (FS-2), shape (3/8c), suture length (75 cm), and suture material (Polyglactin 910). Also provided are an illustration, description (‘undyed braided absorbable suture’), and expiration date. Source: Laurence Jordan, Francois Bronnec, Pierre Machtou.
3.7 Surgical Handpiece and Bur
Conventional dental highand slow-speed handpieces are typically not suitable for dentoalveolar surgery, for several reasons:
https://t.me/DentalBooksWorld

3.8 Surgical Irrigation SSstems 51
Figure 3.15 Frasier suction tip. Source: KLS Martin.
●Air-driven, high-speed handpieces used in dentistry are generally designed with a ‘front-end’ exhaust system; that is, air pressure is released axially near the bur. Use of this type of system under or near periodontal flaps and bone can push large amounts of air and coolant into the soft tissues of the head and neck, resulting in surgical emphysema.
●Slow-speed handpieces do not turn at a sufficient speed or torque to efficiently section a tooth through the enamel and dentine in a controlled fashion.
●Contra-angle handpieces may be used, but in posterior areas their head can limit visualisation of structures.
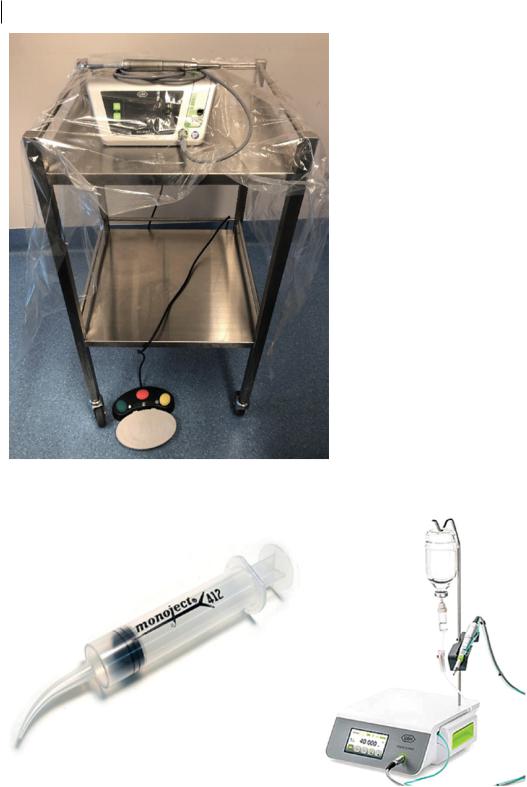
There are several components to a surgical unit: the unit itself, which allows manipulation of the torque and speed; the motor, which is usually a separate component and can be sterilised; and either a foot pedal or an attachment on the handpiece itself, to control the instrument (Figure 3.16).
3.8Surgical Irrigation Systems
Irrigation of a surgical site with sterile saline reduces the amount of remaining debris, may improve healing, and reduce rates of postoperative infection. An efficient suction/irrigation system is also
https://t.me/DentalBooksWorld
52 3 Basic Surgical Instruments
Figure 3.16 Surgical bur setup with sterile plastic and foot pedal.
Figure 3.17 Options for surgical irrigation include use of a Monoject (R) syringe or an irrigation system inbuilt into the surgical drill. Source: Laurence Jordan, Francois Bronnec, Pierre Machtou.
https://t.me/DentalBooksWorld