11 • Imaging of the Liver Post-Surgery and/or Post-Ablative Therapy |
375 |
a |
b |
c |
d |
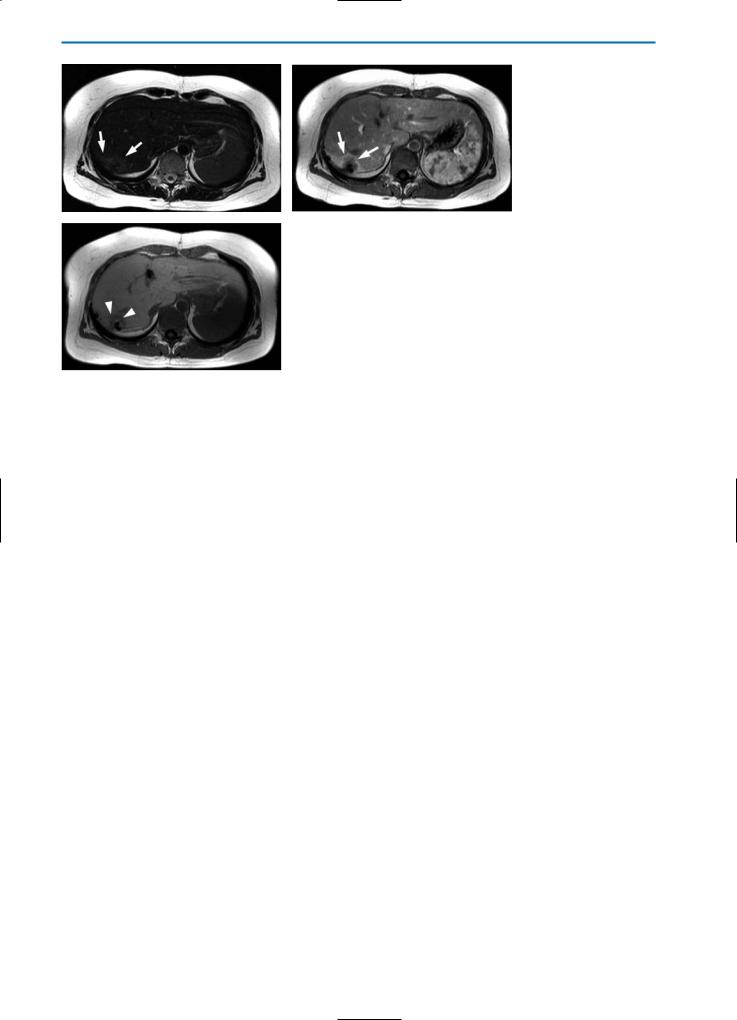
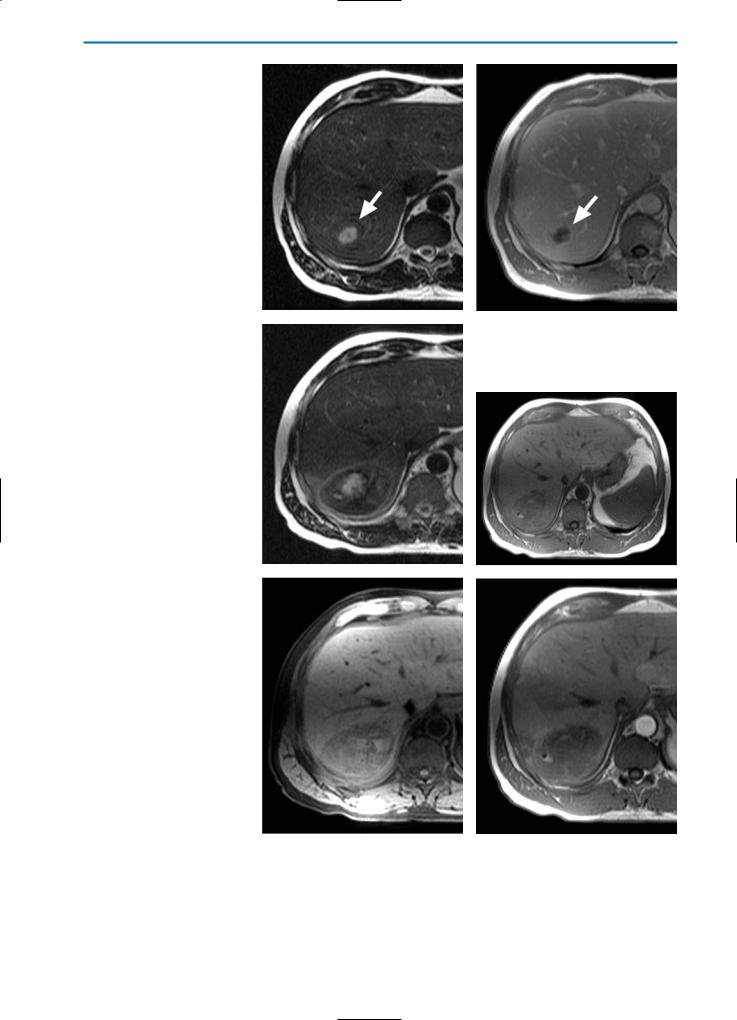
Fig. 4a-d. Patient with solitary metastasis of breast cancer treated with radio-frequency (RF) ablation. Imaging was performed three days after ablation. On the unenhanced T2-weighted HASTE images in axial (a) and coronal (b) orientation, the RF-lesion (arrows) shows a low SI, surrounded by a rim of even lower SI. Note the inflammation of the surrounding liver parenchyma, which has an increased SI. These changes are most likely caused by impairment of hepatic perfusion due to RF-ablation. In the equilibrium phase (c) after contrast agent injection (0.05 mmol/kg BW Gd-BOPTA), T1-weighted images show a closed, hyperintense rim surrounding the lesion. The lesion itself demonstrates no enhancement, indicating complete tumor destruction. In the hepatobiliary phase one hour after Gd-BOPTA administration (d), heterogeneous contrast agent uptake of the liver tissue surrounding the RF-lesion is demonstrated, the lesion shows no enhancement and is sharply demarcated from the surrounding liver
11 • Imaging of the Liver Post-Surgery and/or Post-Ablative Therapy |
377 |
a |
b |
c |
d |
|
e |
f |
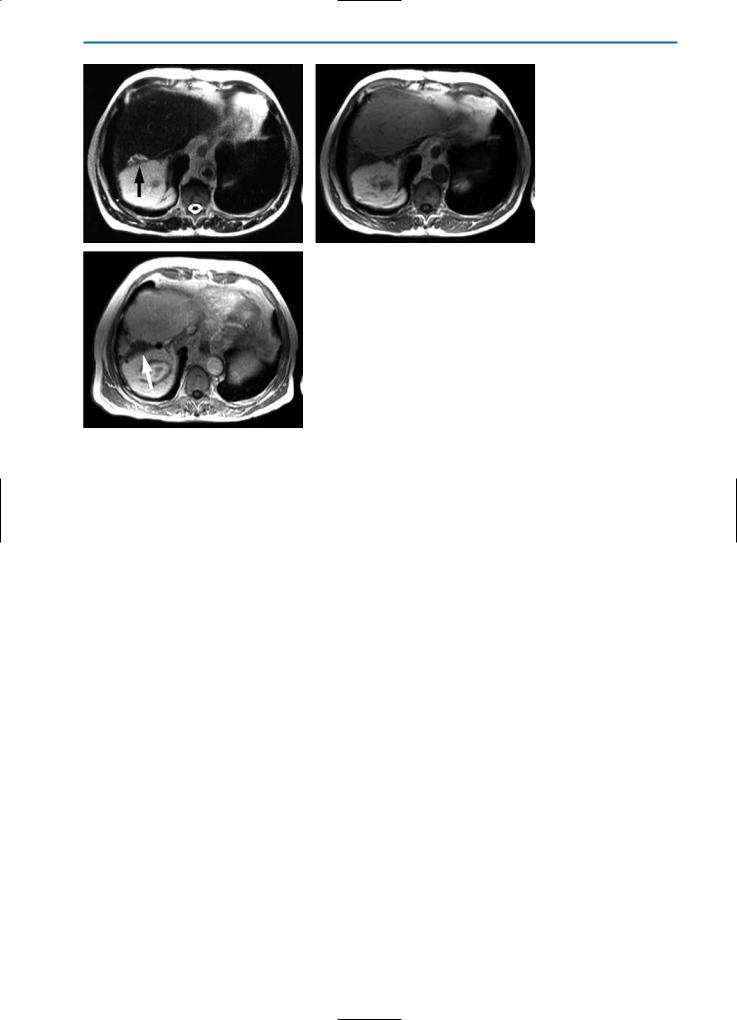
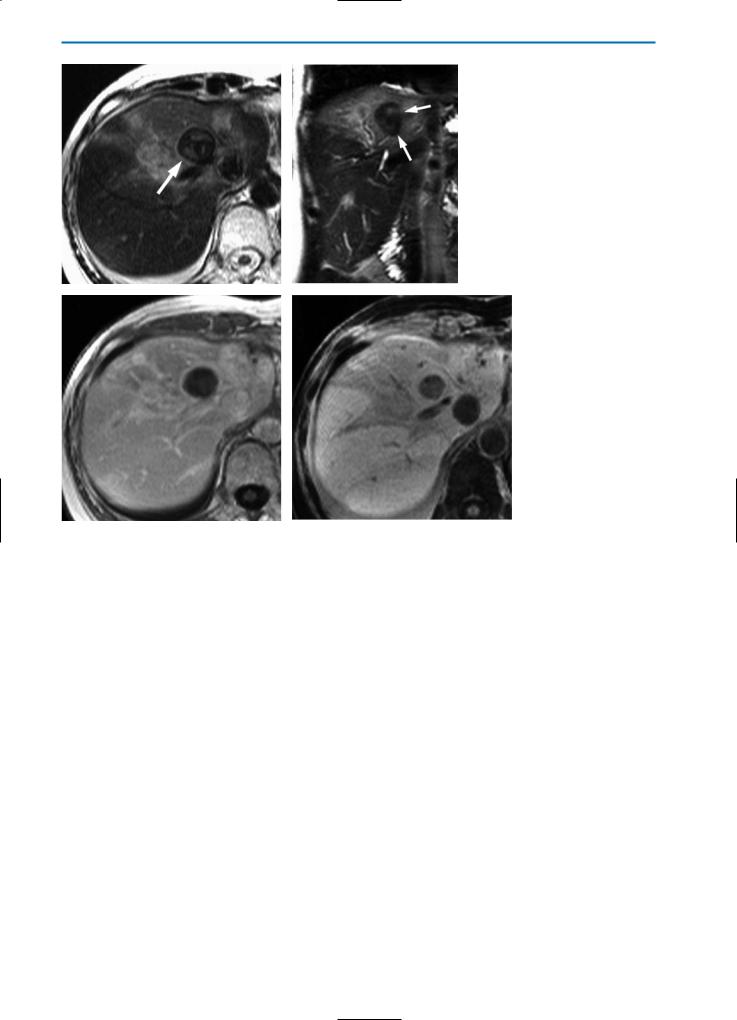
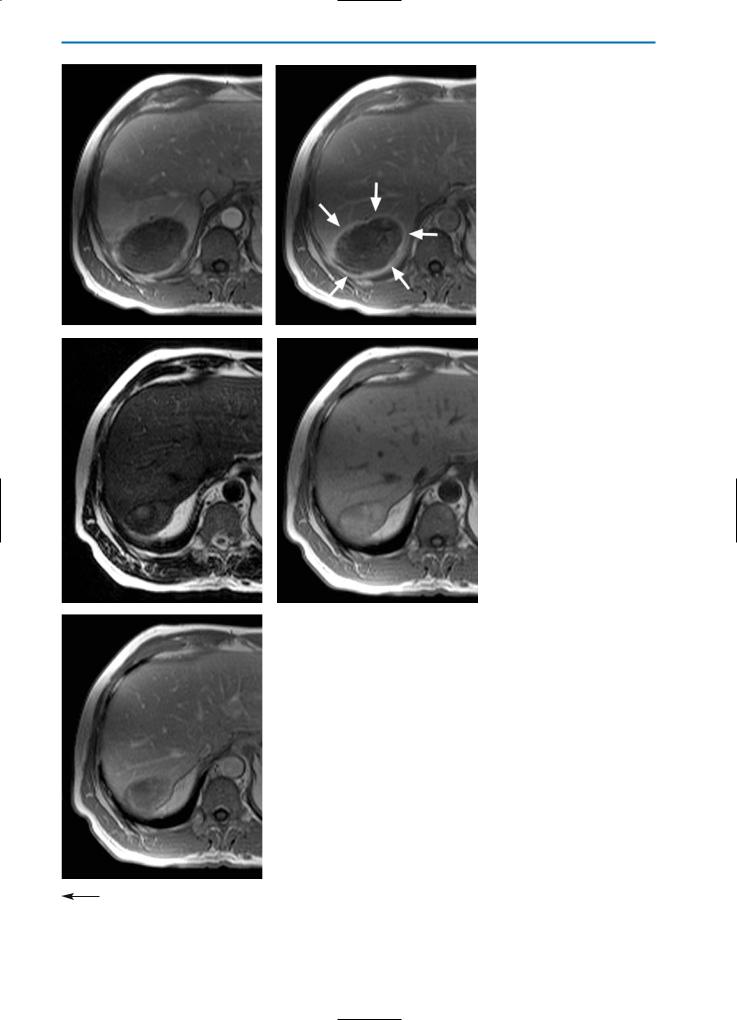
Fig. 6a-f. Patient with metastases from colorectal cancer treated by LITT intervention. The T2-weighted HASTE images in axial (a) and coronal (b) orientation demonstrate a hyperintense lesion (arrow), surrounded by some hypointense tissue which again is demarcated from the normal liver parenchyma by a hyperintense rim. On the corresponding T1-weighted (c) and T1-weighted fat suppressed images
(d) the more peripheral parts of the lesion show signs of hemorrhage (arrow in d). On T1-weighted (e) and T1-weighted fat suppressed (f) images, acquired during the equilibrium phase after contrast agent injection, the lesion is distinguished from surrounding liver tissue by a hyperintense rim. The absence of contrast agent uptake in the center of the lesion indicates complete tumor destruction


11 • Imaging of the Liver Post-Surgery and/or Post-Ablative Therapy |
381 |
g |
h |
i |
j |
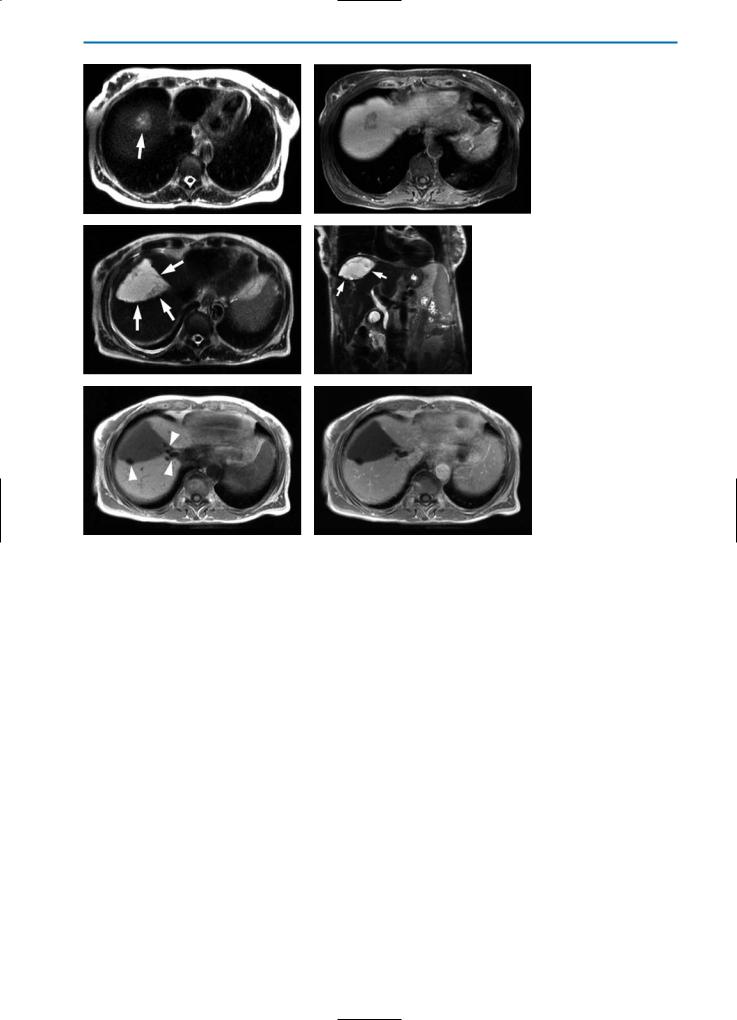
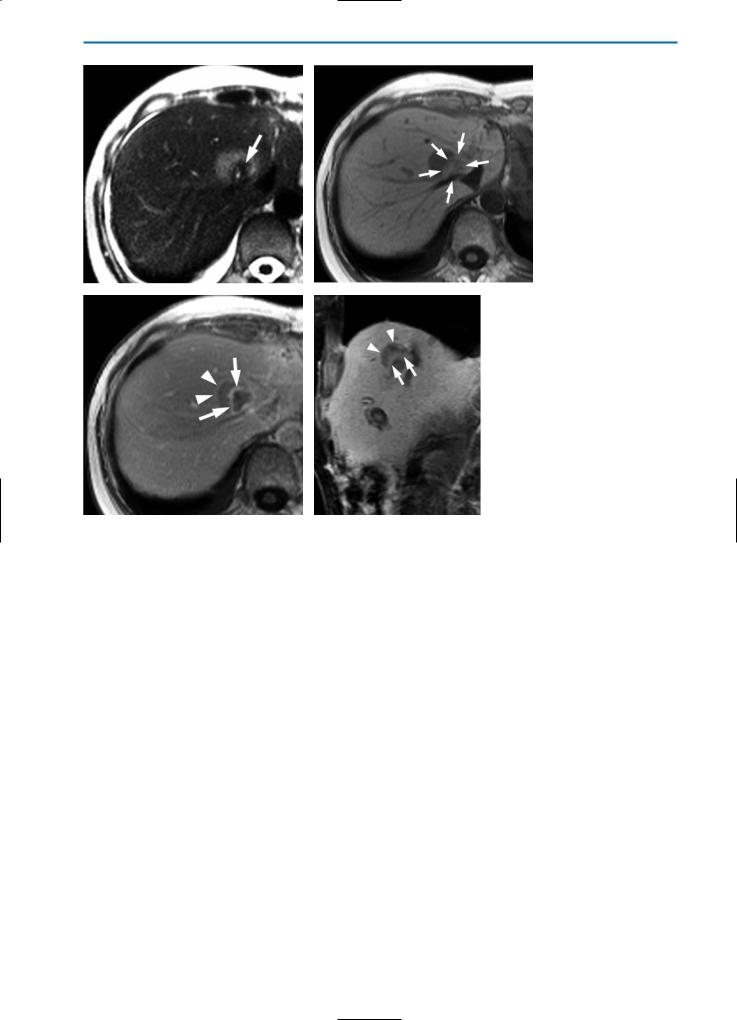
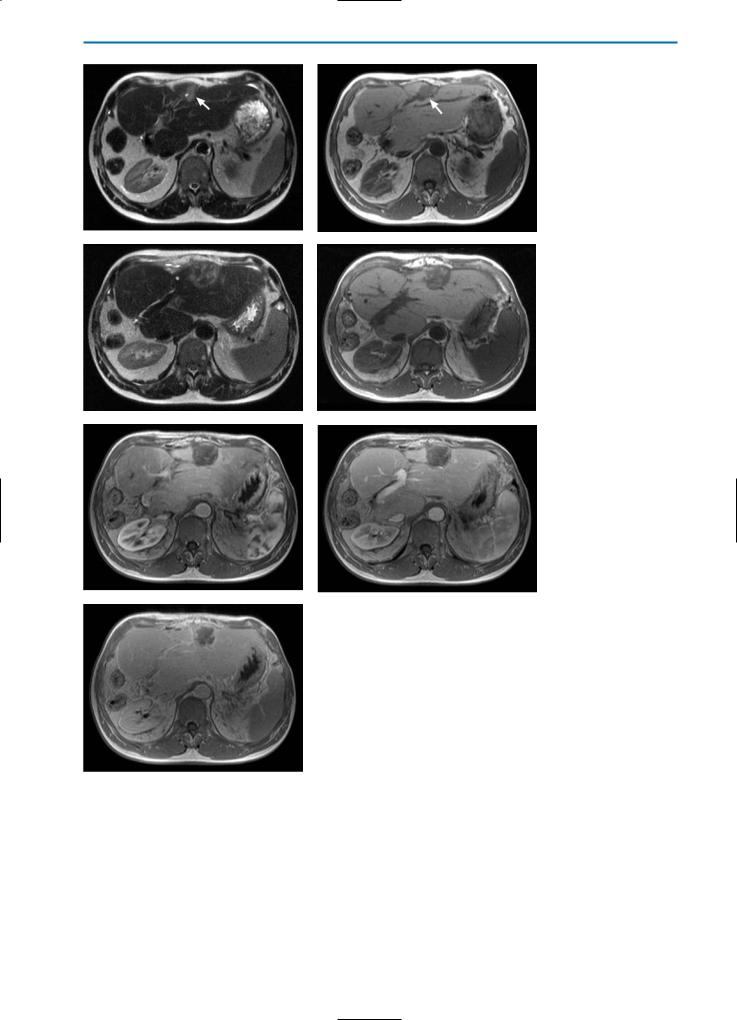
Fig. 7a-k. Liver lesions post-cryotherapy / no residual tumor. Pre-cryotherapy, the T2weighted (a) and contrast-enhanced T1-weighted equilibrium phase (b) images show a partially necrotic metastasis of colorectal cancer (arrows). One week after cryotherapy, the T2-weighted image (c) shows a partially hyperintense, partially hypointense region surrounded by a high SI rim. On the corresponding T1-weighted (d) and T1-weighted fatsuppressed (e) images, high SI areas within the cryolesion can be detected, indicating hemorrhage. Dynamic imaging in the arterial phase (f) reveals segmental hypervascularization of the affected liver segment, which is even more obvious in the portal-venous phase (g). However, no peripheral enhancement of the cryolesion is detected, indicating no residual tumor. In the equilibrium phase (h) a closed hyperintense rim (arrows) surrounding the lesion is observed without any enhancement of central areas. This indicates complete destruction of the tumor tissue.
A T2-weighted image acquired six months after cryotherapy (i) shows that the cryolesion still has heterogeneous, partially high SI. On the corresponding T1-weighted image (j), heterogeneously high SI can be observed. On contrast-enhanced images in the equilibri-
kum phase (k), enhancement of the central areas of the lesion is still not visible and a closed hyperintense rim surrounding the lesion can still be seen
382 MRI of the Liver
a |
b |
c |
d |
e |
f |
g
Fig. 8a-g. Liver lesion post-cryotherapy showing no residual tumor in a patient with previous liver resection.
On the unenhanced T2-weighted (a) and T1-weighted (b) images pre-cryotherapy, a metastasis (arrows) can be seen in the left liver lobe. Note that the patient underwent previous right hemi-hepatectomy. The T2-weighted image (c) acquired one month following cryotherapy, shows a heterogeneous, predominantly high SI lesion. On the T1-weighted image (d), this lesion is hypointense with some high SI areas indicative of hemorrhage. On dynamic imaging, segmental hypervascularization can again be noted in the arterial phase (e) with homogeneous signal in the portal-venous phase (f). The equilibrium phase image (g) again shows a closed hypervascular rim surrounding the lesion, indicating complete destruction of the metastasis
11 • Imaging of the Liver Post-Surgery and/or Post-Ablative Therapy |
383 |
a |
b |
c |
d |
e |
f |
g
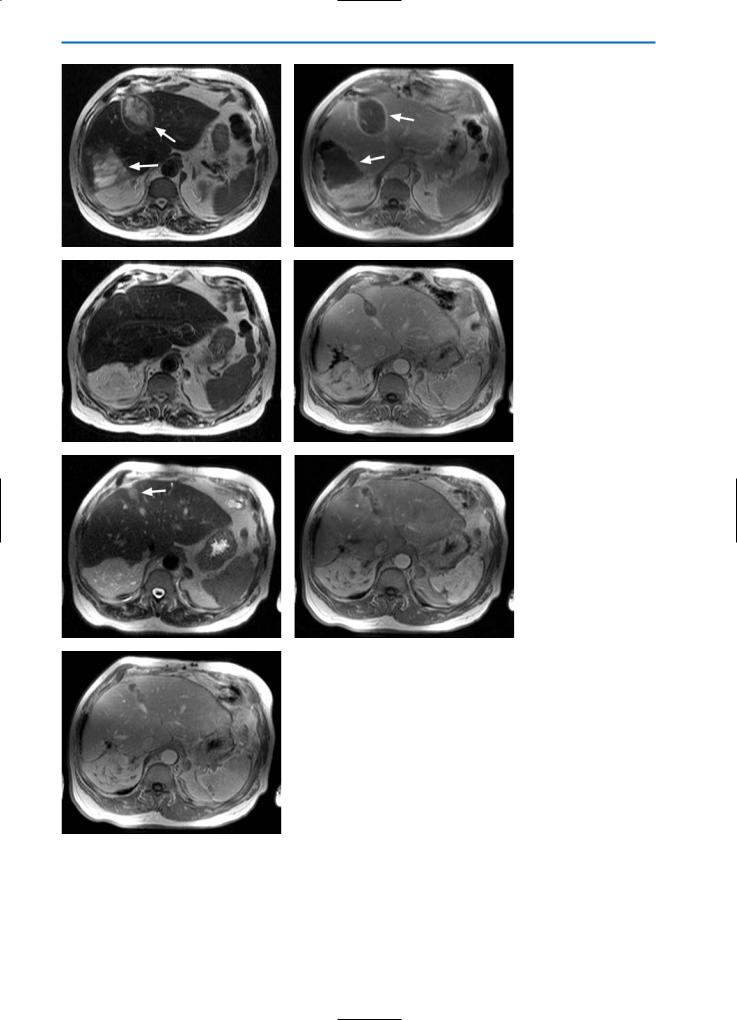
Fig. 9a-g. Patient post-cryotherapy demonstrating late recurrent disease. T2-weighted (a) and contrast-enhanced T1-weighted equilibrium phase (b) images acquired three weeks after cryotherapy show two large cryolesions (arrows). Hyperintense rims surrounding the lesions are apparent on the T1-weighted equilibrium phase image (b). Significant reduction of the size of the cryolesion can be noted on both T2-weighted (c) and contrast-enhanced T1-weighted equilibrium phase (d) images acquired six months post-cryotherapy. No signs of residual tumor or local recurrence are apparent. However, on a T2-weighted image acquired 12 months post-cryotherapy (e), again a homogeneous high SI lesion (arrow) in the area of one of the former cryolesions can be seen. On the corresponding T1-weighted image in the arterial phase after contrast agent injection (f), an irregular peripheral enhancement of the affected region is evident. In the equilibrium phase (g), no hyperintense rim can be observed. Taken together, these observations indicate local recurrent disease
384 MRI of the Liver
a |
b |
c |
d |
e |
f |
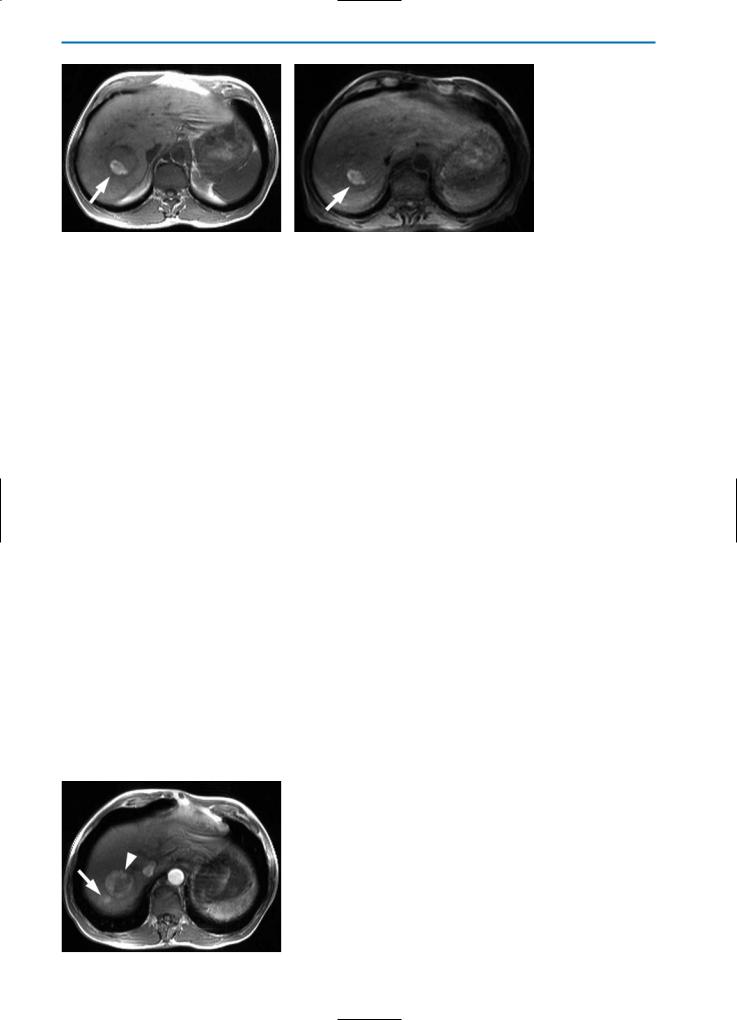
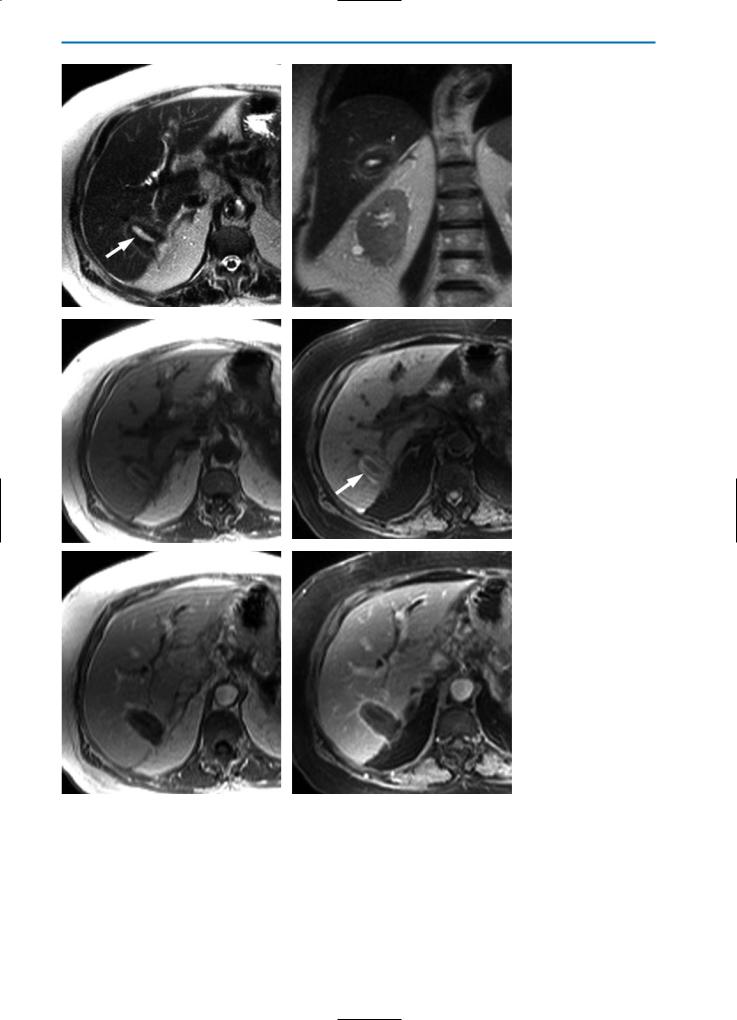
Fig. 10a-f. HCC post-percutaneous ethanol injection (PEI) / residual tumor. The nodule (arrow) appears hypointense with slightly hyperintense peripheral areas on the T2-weighted image (a) and hyperintense on the T1-weighted image (b) after PEI treatment. A focal hypervascular area (arrowhead), representing focal residual tumor, is seen during the arterial phase after the bolus injection of Gd-BOPTA (c). The portal-venous and equilibrium phase images (d and e, respectively) reveal contrast agent wash-out from the residual tumor and an overall hypointense appearance. The delayed hepatobiliary phase image (f) indicates that the residual tumor does not significantly take up Gd-BOPTA. This case is typical of residual tumor in HCC treated by percutaneous ethanol injection. The arterial phase image after contrast agnet injection is most sensitive for the detection of residual or recurrent tumor in cases of HCC or other hypervascular lesions